![]()
![]()

![]()

The goal of {coder} is to classify items from one
dataset, using codes from a secondary source with classification schemes
based on regular expressions and weighted indices.
You can install the released version of coder from CRAN with:
# install.packages("coder")And the development version from GitHub with:
# install.packages("remotes")
remotes::install_github("eribul/coder")Patient data: The initial rationale for the package was to classify patient data based on medical coding. A typical use case would consider patients from a medical/administrative data base, as identified by some patient id and possibly with some associated date of interest (date of diagnoses/treatment/intervention/hospitalization/rehabilitation). This data source could be for example an administrative hospital register or a national quality register.
Codify: The primary source could then be linked to a secondary (possibly larger) data base including the same patients with corresponding id:s and some coded patient data. This could be a national patient register with medical codes from the International Classification of Diseases (ICD) with corresponding dates of hospital visits/admission/discharge, or a medical prescription register with codes from the Anatomic Therapeutic Chemical (ATC) classification system with dates of medical prescription/dispatch/usage. A time window could be specified relating the date of the primary source (i. e. the date of a primary total hip arthroplasty; THA), to dates from the secondary source (i.e. the date of a medical prescription). ATC codes associated with medical prescriptions during one year prior to THA, could thus be identified and used as a measure of comorbidity. Another time window of 90 days after THA, might instead be used to identify adverse events after surgery.
Classify: To work with medical/chemical codes
directly might be cumbersome, since those classifications tend to be
massive and therefore hard to interpret. It is thus common to use data
aggregation as proposed by some classification or combined index from
the literature. This could be the Charlson or
Elixhauser comorbidity indices based on ICD-codes, or the
RxRisk V classification based on ATC-codes. Each of those tools
appear with different code versions (ICD-8, ICD-9, ICD-9-CM, ICD-10,
ICD-10-CA, ICD-10-SE, ICD-10-CM et cetera) and with different codes
recognized as relevant comorbidities (the Charlson index proposed by
Charlson et al, Deyo et al, Romano et al. Quan et al. et cetera). Using
a third object (in addition to the primary and secondary patient data
sets) helps to formalize and structure the use of such classifications.
This is implemented in the coder package by
classcodes objects based on regular expressions (often with
several alternative versions). Those classcodes objects
could be prepared by the user, although a number of default
classcodes are also included in the package (table
below).
Index: Now, instead of working with tens of thousands of individual ICD-codes, each patient might be recognized to have none or some familiar comorbidity such as hypertension, cancer or dementia. This granularity might be too fine-grained still, wherefore an even simpler index score might be searched for. Such scores/indices/weighted sums have been proposed as well and exist in many versions for each of the standard classifications. Some are simple counts, some are weighted sums, and some accounts for some inherited hierarchy (such that ICD-codes for diabetes with and without complications might be recognized in the same patient, although the un-complicated version might be masked by the complicated version in the index).
Conditions: Some further complexity might appear if some codes are only supposed to be recognized based on certain conditions. Patients with THA for example might have an adverse event after surgery if a certain ICD-code is recorded as the main diagnose at a later hospital visit, although the same code could be ignored if recorded only as a secondary diagnosis.
To summarize: The coder package takes three objects:
(1) a data frame/table/tibble with id and possible dates from a primary
source; (2) coded data from a secondary source with the same id and
possibly different dates and; (3) a classcodes object,
either a default one from the package, or as specified by the user. The
outcome is then: (i) codes associated with each element from (1)
identified from (2), possibly limited to a relevant time window; (ii) a
broader categorization of the relevant codes as prescribed by (3), and;
(iii) a summarized index score based on the relevant categories from
(3).
(i-iii) corresponds to the output from functions
codify(), classify() and index(),
which could be chained explicitly as
codify() %>% classify() %>% index(), or implicitly by
the categorize() function.
Assume we have some patients with surgery at specified dates:
library(coder)
ex_people
#> # A tibble: 100 × 2
#> name surgery
#> <chr> <date>
#> 1 Chen, Trevor 2022-08-12
#> 2 Graves, Acineth 2022-05-04
#> 3 Trujillo, Yanelly 2022-04-21
#> 4 Simpson, Kenneth 2022-07-24
#> 5 Chin, Nelson 2022-07-07
#> 6 Le, Christina 2022-02-08
#> 7 Kang, Xuan 2022-05-13
#> 8 Shuemaker, Lauren 2022-02-09
#> 9 Boucher, Teresa 2022-07-18
#> 10 Le, Soraiya 2022-06-22
#> # … with 90 more rowsThose patients (among others) were also recorded in a national patient register with date of hospital admissions and diagnoses codes coded by the International Classification of Diseases (ICD) version 10:
ex_icd10
#> # A tibble: 2,376 × 4
#> name admission icd10 hdia
#> <chr> <date> <chr> <lgl>
#> 1 Tran, Kenneth 2022-02-23 S134A FALSE
#> 2 Tran, Kenneth 2022-08-09 W3319 FALSE
#> 3 Tran, Kenneth 2022-07-19 Y0262 TRUE
#> 4 Tran, Kenneth 2022-06-11 X0488 FALSE
#> 5 Sommerville, Dominic 2022-07-31 V8104 FALSE
#> 6 Sommerville, Dominic 2022-03-11 B853 FALSE
#> 7 Sommerville, Dominic 2022-07-26 Q174 FALSE
#> 8 Sommerville, Dominic 2022-03-16 A227 FALSE
#> 9 Sommerville, Dominic 2022-07-21 H702 FALSE
#> 10 Sommerville, Dominic 2021-11-12 X6051 TRUE
#> # … with 2,366 more rowsUsing those two data sets, as well as a classification scheme
(classcodes object; see below), we can easily identify all
Charlson comorbidities for each patient:
ch <-
categorize(
ex_people, # patients of interest
codedata = ex_icd10, # Medical codes from national patient register
cc = "charlson", # Calculate Charlson comorbidity
id = "name", code = "icd10" # Specify column names
)
#> Classification based on: icd10
ch
#> # A tibble: 100 × 25
#> name surgery myocardial.infarction congestive.heart.failure peripheral.vascular.disease cerebrovascular.dise…¹ demen…² chron…³ rheum…⁴ pepti…⁵ mild.…⁶ diabe…⁷ hemip…⁸ renal…⁹ diabe…˟ malig…˟ moder…˟ metas…˟ AIDS.…˟ charl…˟ deyo_…˟ dhoore ghali quan_…˟ quan_…˟
#> <chr> <date> <lgl> <lgl> <lgl> <lgl> <lgl> <lgl> <lgl> <lgl> <lgl> <lgl> <lgl> <lgl> <lgl> <lgl> <lgl> <lgl> <lgl> <dbl> <dbl> <dbl> <dbl> <dbl> <dbl>
#> 1 Chen, Trevor 2022-08-12 FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE 0 0 0 0 0 0
#> 2 Graves, Acineth 2022-05-04 FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE 0 0 0 0 0 0
#> 3 Trujillo, Yanelly 2022-04-21 FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE 0 0 0 0 0 0
#> 4 Simpson, Kenneth 2022-07-24 FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE 0 0 0 0 0 0
#> 5 Chin, Nelson 2022-07-07 FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE 0 0 0 0 0 0
#> 6 Le, Christina 2022-02-08 FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE TRUE FALSE FALSE FALSE 2 1 1 0 2 2
#> 7 Kang, Xuan 2022-05-13 FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE 0 0 0 0 0 0
#> 8 Shuemaker, Lauren 2022-02-09 FALSE FALSE FALSE FALSE FALSE TRUE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE 1 1 1 0 1 1
#> 9 Boucher, Teresa 2022-07-18 FALSE FALSE TRUE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE 1 1 1 2 1 0
#> 10 Le, Soraiya 2022-06-22 FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE FALSE 0 0 0 0 0 0
#> # … with 90 more rows, and abbreviated variable names ¹cerebrovascular.disease, ²dementia, ³chronic.pulmonary.disease, ⁴rheumatic.disease, ⁵peptic.ulcer.disease, ⁶mild.liver.disease, ⁷diabetes.without.complication, ⁸hemiplegia.or.paraplegia, ⁹renal.disease,
#> # ˟diabetes.complication, ˟malignancy, ˟moderate.or.severe.liver.disease, ˟metastatic.solid.tumor, ˟AIDS.HIV, ˟charlson, ˟deyo_ramano, ˟quan_original, ˟quan_updatedHow many patients were diagnosed with malignancy?
sum(ch$malignancy)
#> [1] 5What is the distribution of the combined comorbidity index for each patient?
barplot(table(ch$charlson))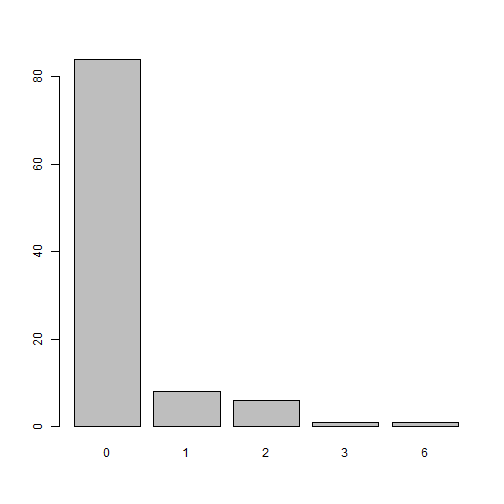
There are many versions of the Charlson comorbidity index, which
might be controlled by the index argument. We might also be
interested only in diagnoses from 90 days before surgery as specified
with an argument list codify_argsas passed to
codify():
ch <-
categorize(
ex_people, codedata = ex_icd10, cc = "charlson", id = "name", code = "icd10",
# Additional arguments
index = c("quan_original", "quan_updated"), # Indices
codify_args = list(
date = "surgery", # Name of column with index dates
code_date = "admission", # Name of column with code dates
days = c(-90, -1) # Time window
)
)
#> Classification based on: icd10Number of malignancies during this period?
sum(ch$malignancy, na.rm = TRUE)
#> [1] 3Distribution of the index as proposed by Quan et al 2011 during the 90 day period:
barplot(table(ch$quan_updated))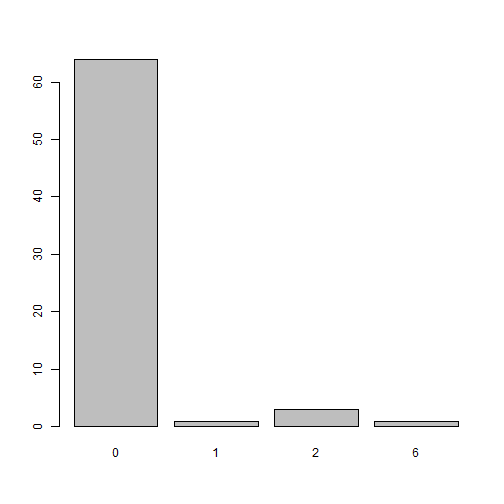
Classification schemes (classcodes objects, see
vignette("classcodes")) are based on regular expressions
for computational speed (see
vignette("Interpret_regular_expressions")), but their
content can be summarized and visualized for clarity. Arbitrary
classcodes objects can also be specified by the user.
The package includes default classcodes for medical
patient data based on the international classification of diseases
version 8, 9 and 10 (ICD-8/9/10), as well as the Anatomical Therapeutic
Chemical Classification System (ATC) for medical prescription data.
Default classcades are listed in the table. Each
classification (classcodes column) can be based on several code systems
(regex column) and have several alternative weighted indices (indices
column). Those might be combined freely.
coder::all_classcodes()
#> # A tibble: 7 × 3
#> classcodes regex indices
#> <chr> <chr> <chr>
#> 1 charlson icd10, icd9cm_deyo, icd9cm_enhanced, icd10_rcs, icd8_brusselaers, icd9_brusselaers "charlson, deyo_ramano, dhoore, ghali, quan_original, quan_updated"
#> 2 cps icd10 "only_ordinary"
#> 3 elixhauser icd10, icd10_short, icd9cm, icd9cm_ahrqweb, icd9cm_enhanced "sum_all, sum_all_ahrq, walraven, sid29, sid30, ahrq_mort, ahrq_readm"
#> 4 hip_ae icd10, kva, icd10_fracture ""
#> 5 hip_ae_hailer icd10, kva ""
#> 6 knee_ae icd10, kva ""
#> 7 rxriskv atc_pratt, atc_caughey, atc_garland "pratt, sum_all"coder uses data.table as a backend to
increase computational speed for large datasets. There are some R
packages with a narrow focus on Charlson and Elixhauser co-morbidity
based on ICD-codes (icd, comorbidity,
medicalrisk,
comorbidities.icd10,
icdcoder). The
coder package includes similar functionalities but has a
wider scope.
Please note that this package is released with a Contributor Code of Conduct. By contributing to this project, you agree to abide by its terms.